|
|
||
|
|
Note. This page may take time to download.
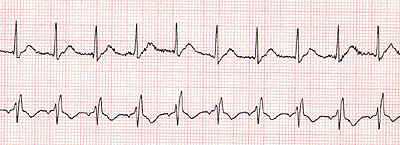
Left Bundle Branch Block
The
QRS complex represents the amount of time required to depolarize the
ventricles. A normal QRS is 0.08-0.12 seconds in length. A length
greater than 0.12 seconds is considered a BBB. This means that there may
be a block in one of the bundle branches, or the electrical impulse was
conducted through an abnormal conduction pathway. This can occur in any
rhythm. The causes range from normal to pericarditis, myocarditis,
congested heart failure and congenital heart disease. Rate:
Atrial and ventricular rate can vary depending on the specific rhythm
involved. Any rhythm can have BBB. The P Wave depends on the intrinsic
rhythm involved. The QRS is the determining factor and it must be
greater than 0.12 seconds.
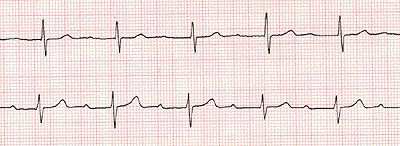
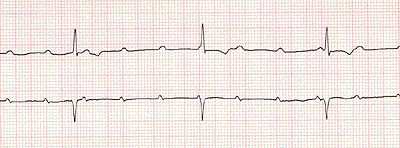
First Degree AV Block
Definition: 1AVB is
a rhythm in which the electrical impulse which leaves the SA node and
travels through the atria, AV node, Bundle of His to purkininjie fibers
is slowed down and takes longer than normal to arrive at its
destination. The normal PR interval is 0.12- 0.20 seconds. A 1AVBT is
greater than 0.20 seconds. The cause ranges from coronary heart disease,
inferior wall MI's, hyperkalemia, congenital abnormalities, and
medications such as quinidine,
digitalis, beta blockers, and
calcium channel blockers. Rate: The atrial rate or P waves can vary to any rate. The ventricular rate can also vary. There must be a 1:1 conduction of the P waves to the QRS waves. Rhythm: Atrial and ventricular rates are usually regular, but they may also be irregular. P Wave: Usually normally shaped and occurring with a 1:1 ration with the QRS. PR interval: greater than0.20 seconds. QRS Complex: Within normal limits or may have a bundle branch block. ST Segment: Within normal limits for the intrinsic rhythm. T Wave: Within normal size and configuration.
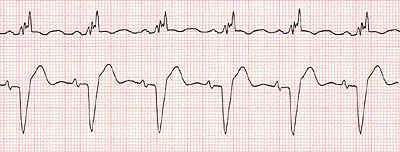
Second degree AV Block type 1 (Mobitz).
Second degree AV Block Type II
Definition:
Second
degree AV block is also known as Second Degree Type I, Mobitz I,
or Wenckelbach. This arrhythmia is characterized by a progressive delay
of the conduction at the AV node, until the conduction is completely
blocked. This occurs because the impulse arrives during the absolute
refractory period, resulting in an absence of conduction, and no QRS.
The next P wave occurs and the cycle begins again. Possible causes are
acute inferior wall myocardial infraction, digitalis, beta blockers,
calcium channel blockers, rheumatic fever, myocarditis, or excessive
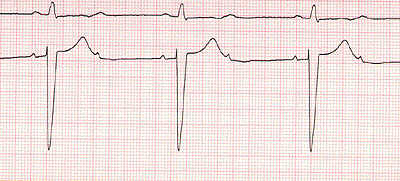
vagal tone. Rate is ususaly 60-100 beats per minute. Atrial rhythm is regular. Ventricular rhythm is irregular. P Wave configuration is normal. PR interval gets longer with each beat until QRS complex is dropped. QRS complex is normal, but is dropped periodically. ST Segment and T Wave are normal in configuration. Ventricular rate will depend on the number of impulses conducted through the AV node, and will be less than the atrial rate. Rhythm: Atrial and ventricular rate is irregular. P Wave: Present in two, three or four to one conduction with the QRS. PR Interval: Constant for each P wave proir to the QRS. QRS: May be within normal limits for the intrinsic rhythm. ST Segment: Normal in size and configuraration. Third Degree. Complete Block
A third degree atrial ventricular block is also know as a complete heart block artrioventricular block of 3degree AV block. It is a problem with electrical conduction. All electrical conduction from the atria are blocked at the AV junction, therefore, the atria and the ventricles beat independently from each other. This arrhythmia is dangerous because it significantly decreases cardiac output, and could lead to asystole. Possible causes: acute inferior and anterior myocardic infraction, coronary heart disease, excessive vagal tone, myocarditis, endocarditis, age, edema from heart surgery, and meditation toxicity from digitalis, beta blockers, calcium channel blockers Atrial rate faster than ventricular rate. Rhythm: Regular, but there is normal configuration. PR Interval: There is no relationship between P waves and QRS complexes. QRS Complex: Variates depending on the intrinsic rhythm. ST Segment and T Wave: Normal configurations ST segment elevation is usually attributed to impending infarction, but can also be due to pericarditis or vasospastic (variant) angina. In some healthy young adults, a form of ST elevation can be normal. The height of the ST segment is measured at a point 2 boxes after the end of the QRS complex. ST segment elevation is considered significant if it exceeds 1 mm in a limb lead or 2 mm in a precordial lead. Infarction In transmural infarction, ST segment elevation will be among the first manifestations. The ST segment elevation will be seen in those leads involved in impending infarction. ST segment elevation decreases as T wave inversion begins. ST segments may remain elevated when ventricular aneurysm develops. ST segment elevation that persists beyond three months following myocardial infarction suggests ventricular aneurysm. ST elevation will be present in about 1/3 of ventricular aneurysms. When the patient with ventricular aneurism presents with acute chest pain, a baseline ECG may help avoid misdiagnosis of impending infarction (and use of non-needed thrombolytic drugs). Vasospastic angina ST segment elevation can be seen in a severe type of ischemia called vasospastic or Prinzmetal’s angina. While exercise angina involves the subendocardium, vasospastic angina causes severe transmural loss of blood flow. ST elevation simply indicates injury, whether due to coronary thrombosis with impending infarction, or coronary spasm (Prinzmetal’s angina). At this point, the injury is reversible. Pericarditis: Pericarditis, an inflammation of the
space between the pericardial sack and outer surface of the heart,
causes widespread ST segment elevation. Physical damage and irritation
of the heart’s surface produces a “current of injury” in virtually
all ECG leads. Later in the course of pericarditis, ST segment elevation resolves, without development of Q waves. After days to months, ST elevation is replaced by widespread T wave inversions. “Early repolarization” is a cause of ST elevation. This innocent condition typically occurs in young healthy males. The T wave begins early, adding elevation to the ST segment. Usually, early repolarization shows elevation of the J point (the junction between the end of the QRS and the ST segment) and a concave upward curve towards the T wave. (“Concave upward” means the hollow portion of the curve is on top.) Early repolarization is usually
seen in the anterior precordial leads of the ECG, but can be seen in
limb leads to a lesser degree. |
|